Jaw Pain
Jaw Pain from Wisdom Teeth vs TMJ: Key Differences
Jaw Pain from Wisdom Teeth vs TMJ: Key Differences article.
Jaw pain is one of the most common complaints I see in my oral surgery practice, and among the most frequently misidentified causes are wisdom teeth problems and TMJ disorders. Patients routinely confuse the two — not surprising, given that both produce pain in the jaw area, can cause swelling, and may affect your ability to open your mouth comfortably. But the underlying causes, diagnostic approach, and treatment are fundamentally different. Getting the diagnosis right is the critical first step toward effective treatment. This guide walks you through the key distinguishing features, the clinical evaluation process, and what to expect from each condition.
This article is for informational purposes and is not a substitute for professional dental or medical diagnosis. If you are experiencing jaw pain, please consult a dentist or oral healthcare provider.
Table of Contents
- Understanding the Anatomy: Where the Pain Originates
- What Causes Wisdom Tooth Pain
- What Causes TMJ Pain
- Side-by-Side Comparison: Wisdom Teeth vs TMJ
- How Dentists and Oral Surgeons Diagnose Jaw Pain
- Common Co-Occurrence: Wisdom Teeth and TMJ Together
- Treatment Approaches for Each Condition
- When to Seek Emergency Care
- Frequently Asked Questions
- Sources & Methodology
- About the Author
Understanding the Anatomy: Where the Pain Originates
To understand why wisdom tooth pain and TMJ pain are often confused, it helps to visualize the anatomy.
The Wisdom Teeth
Wisdom teeth — your third and final set of molars — typically erupt between ages 17 and 25. Most adults have four wisdom teeth, one in each corner of the mouth: two in the upper jaw (maxilla) and two in the lower jaw (mandible). Each wisdom tooth sits at the terminus of the dental arch, surrounded by dense gum tissue and in close proximity to the second molars.
Because wisdom teeth are the last to erupt and the jaw has often stopped growing by the time they emerge, there is frequently insufficient space for them to come in properly. This is why impaction — where the tooth fails to fully emerge — is so common with wisdom teeth.
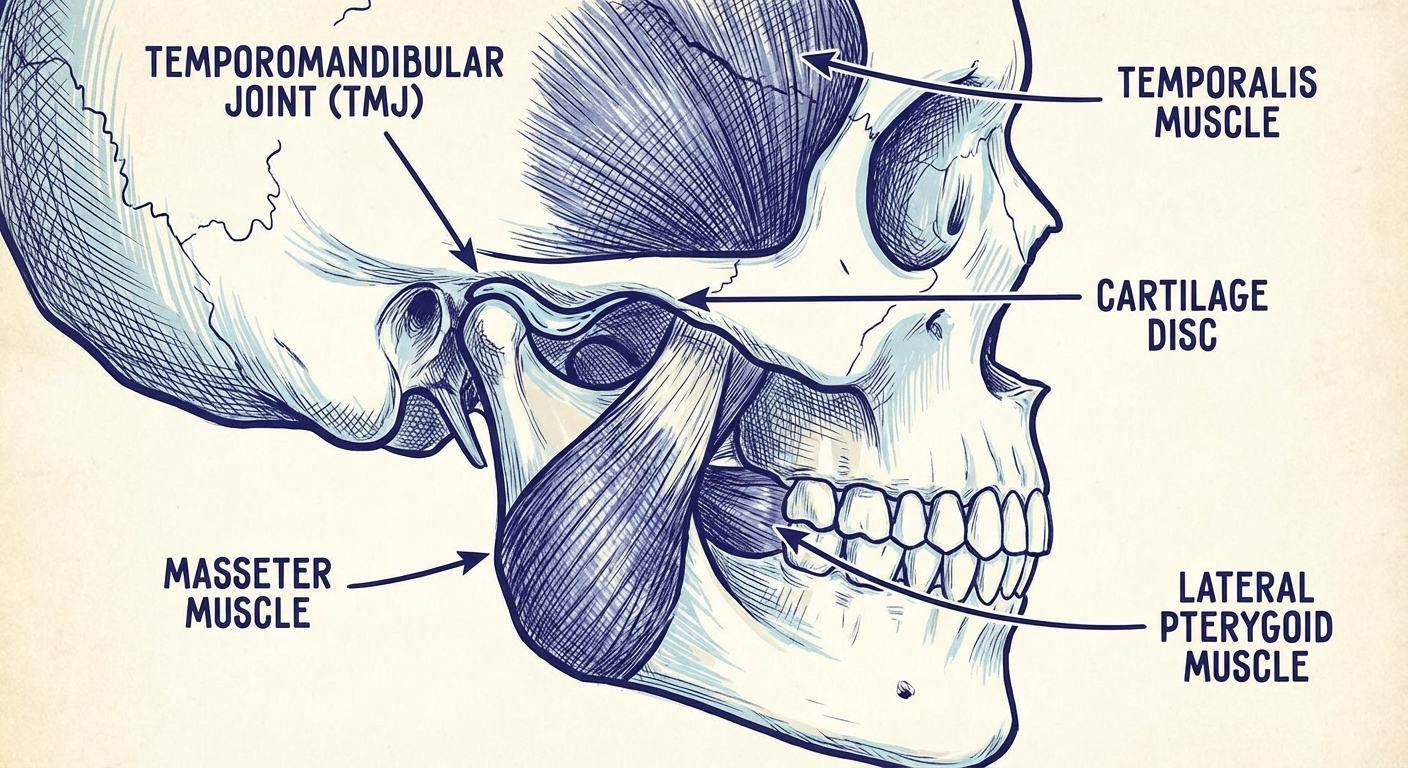
The Temporomandibular Joint (TMJ)
The TMJ is the hinge joint that connects your lower jaw (mandible) to your skull. It is located just in front of each ear canal — you can feel it move if you place your fingers there while opening and closing your mouth. Unlike a simple hinge joint like your knee, the TMJ is a complex joint that allows sliding, hinging, and lateral movement. It is the most complex joint in the human body.
The TMJ includes:
- The condyle (the ball at the top of the mandible)
- The glenoid fossa (the socket in the temporal bone)
- The articular disc (the cartilage cushion between ball and socket)
- Multiple ligaments and muscles (masseter, temporalis, lateral pterygoid, medial pterygoid)
Pain in the TMJ can originate from any of these structures — the muscles, the disc, the ligaments, or the bony surfaces themselves.
Why the Confusion Is Anatomically Understandable
The upper wisdom teeth sit directly adjacent to the muscles of mastication (chewing muscles) that are also involved in TMJ function. Inflammation from a developing or impacted wisdom tooth can irritate these muscles, producing pain that feels like it originates from the joint itself. Similarly, a TMJ disorder that causes altered bite patterns can create uneven pressure on the back molars, potentially triggering wisdom tooth symptoms.
What Causes Wisdom Tooth Pain
Impaction
Impaction occurs when there is insufficient space in the jaw for the wisdom tooth to erupt fully into a functional position. There are several types of impaction:
- Mesial impaction: The tooth is angled forward, toward the second molar. This is the most common type.
- Horizontal impaction: The tooth is lying on its side, fully beneath the gum line, pressing against the second molar roots.
- Vertical impaction: The tooth is nearly upright but fails to fully erupt through the gum.
- Distal impaction: The tooth is angled backward, away from the second molar. This is the least common type.
Impaction does not always cause pain. A deeply impacted wisdom tooth that is entirely below the gum line may be asymptomatic for years and only discovered incidentally on a dental X-ray. Pain typically arises when the impaction creates conditions that lead to inflammation, infection, or pressure damage.
Pericoronitis
Pericoronitis is inflammation of the soft tissue (gingiva) surrounding a partially erupted tooth. When a wisdom tooth breaks through the gum but cannot fully emerge, a flap of gum tissue (called an operculum) remains over a portion of the crown. Food debris and bacteria accumulate under this flap, causing inflammation that can range from mild discomfort to a painful, swollen infection.
Pericoronitis is the most common cause of acute wisdom tooth pain in young adults. It is particularly common in lower wisdom teeth due to the angle of eruption and the thickness of the overlying gum tissue.
Symptoms of pericoronitis include:
- Throbbing pain in the back of the mouth behind the second molar
- Swelling of the gum tissue over the partially erupted tooth
- Pain when swallowing
- Difficulty opening the mouth fully (trismus)
- Referred pain to the jaw, ear, or side of the face
- Sometimes: bad breath (halitosis) or an unpleasant taste from the infected site
Tooth Decay in Wisdom Teeth
Even wisdom teeth that fully erupt are difficult to clean — their position at the back of the mouth makes brushing and flossing challenging. As a result, wisdom teeth have disproportionately high rates of tooth decay (caries). Decay in a wisdom tooth can cause pain that radiates to the jaw, ear, and temple, mimicking TMJ pain.
Decay in a partially erupted wisdom tooth can also progress rapidly because the area is hard to clean and bacteria can accumulate in the gum flap.
Cyst Formation
In rare cases, a wisdom tooth that fails to erupt can lead to cyst formation in the jawbone. A periapical cyst or dentigerous cyst can develop from the dental follicle surrounding the unerupted tooth, gradually expanding and causing jaw swelling, bone destruction, and pain. Cysts require surgical treatment (enucleation) and are typically identified on panoramic X-ray.
What Causes TMJ Pain
TMJ Disorders: An Umbrella Term
"Temporomandibular joint disorders" (TMD) is actually an umbrella term covering several distinct conditions that affect the jaw joint and the surrounding muscles. According to the National Institute of Dental and Craniofacial Research (NIDCR), approximately 10 million Americans are affected by TMD, with women of childbearing age being significantly more likely to seek treatment than men.
Myofascial Pain Dysfunction (MPD)
The most common TMJ disorder is myofascial pain dysfunction, which originates in the muscles that control jaw movement rather than in the joint itself. MPD is characterized by:
- Pain or tenderness in the masseter muscles (the large muscles on the sides of your jaw)
- Pain in the temporalis muscles (above your ears)
- Referred pain to the neck, shoulders, and upper back
- Pain that worsens with jaw function (chewing, talking, yawning)
- No visible joint sounds or only mild clicking
MPD is frequently associated with parafunctional habits — clenching, grinding (bruxism), nail-biting, or resting your jaw on your hand. It is also associated with stress, which tends to increase unconscious clenching. For pain that radiates into the neck and shoulders, targeted relief for related muscle tension can help address secondary muscle guarding alongside TMJ. TMJ pain spreading toward the ear canal is frequently accompanied by tinnitus or a feeling of fullness — addressing TMJ symptoms can also reduce these ear-related manifestations.
Internal Derangement
Internal derangement refers to a mechanical problem within the TMJ itself — most commonly displacement of the articular disc. The disc normally sits between the condyle and the fossa, cushioning the joint and allowing smooth movement. When the disc slips forward (anterior disc displacement), it can:
- Cause a pronounced click or pop when opening or closing the mouth
- Produce a catching or locking sensation mid-opening
- Eventually lead to cartilage breakdown and bone-on-bone contact (osteoarthritis of the TMJ)
Internal derangement is not caused by wisdom teeth. It is caused by ligament laxity, trauma to the jaw (such as a whiplash injury), or repetitive joint overload from chronic clenching.
Degenerative Joint Disease (Osteoarthritis of the TMJ)
Osteoarthritis of the TMJ is wear-and-tear damage to the joint cartilage. It is more common in older adults but can develop at any age in people with chronic TMJ disorders. Symptoms include:
- Crepitus (a grating or grinding sound) during jaw movement
- Progressive loss of jaw opening capacity
- Morning jaw stiffness that improves throughout the day
- Pain that worsens with prolonged chewing
Hypermobility
Some people have TMJ joints that move beyond the normal range — a condition called hypermobility or hyperlaxity. This can cause the jaw to partially dislocate when opening wide (such as during dental treatment or yawning), producing a loud click and significant pain. Hypermobility is typically managed with physical therapy to strengthen the joint stabilizing muscles.
Side-by-Side Comparison: Wisdom Teeth vs TMJ
Quick Reference Table
| Characteristic | Wisdom Tooth Pain | TMJ Pain |
|---|---|---|
| Primary location | Back of mouth, behind second molars | Directly in front of ear (TMJ point) |
| Radiation pattern | Radiates toward ear, jaw angle, neck | Radiates to temple, ear, side of face, neck |
| Triggers | Chewing, particularly hard or chewy foods | Jaw movement, stress, cold air, yawning |
| Opening the mouth | May be limited due to gum swelling (pericoronitis) | Often limited due to joint/muscle restriction |
| Jaw sounds | Rare | Common: clicking, popping, or crepitus |
| Swelling | Common with infection; visible gum swelling | Rare; if present, suggests joint effusion |
| Gum appearance | Red, swollen gum over partially erupted tooth | Normal gums; no visible abnormality |
| Tooth sensitivity | Common near the affected wisdom tooth | Uncommon |
| Worst time of day | Often worse at night due to reclined position | Often worse upon waking (morning clenching) — poor sleep quality from jaw pain compounds the problem; addressing sleep quality is an underutilized part of TMJ management |
| Duration | Days to weeks if caused by pericoronitis; resolves with treatment | Chronic, recurring, or progressive over months to years |
| Age of onset | Typically 17–25 years | Any age; peak onset 20–40 years |
How Dentists and Oral Surgeons Diagnose Jaw Pain

A proper diagnosis of jaw pain requires both clinical evaluation and imaging. Here is what to expect:
Clinical Examination
Your dentist or oral surgeon will begin with a thorough history and physical examination:
History questions may include:
- When did the pain begin?
- What makes the pain better or worse?
- Do you notice jaw clicking, popping, or locking?
- Do you grind or clench your teeth, especially at night?
- Have you had any recent dental work or jaw injuries?
- Do you feel pain when chewing, yawning, or speaking?
Physical examination may include:
- Palpation of the TMJ bilaterally (both sides) while you open, close, and move your jaw side to side
- Assessment of jaw opening range (normal is approximately 35–55 mm, measured between upper and lower incisors)
- Palpation of the masseter and temporalis muscles for tenderness
- Visual inspection of the back molars and gums for signs of wisdom tooth eruption or pericoronitis
- Assessment of your bite (occlusion) for signs of tooth wear from grinding
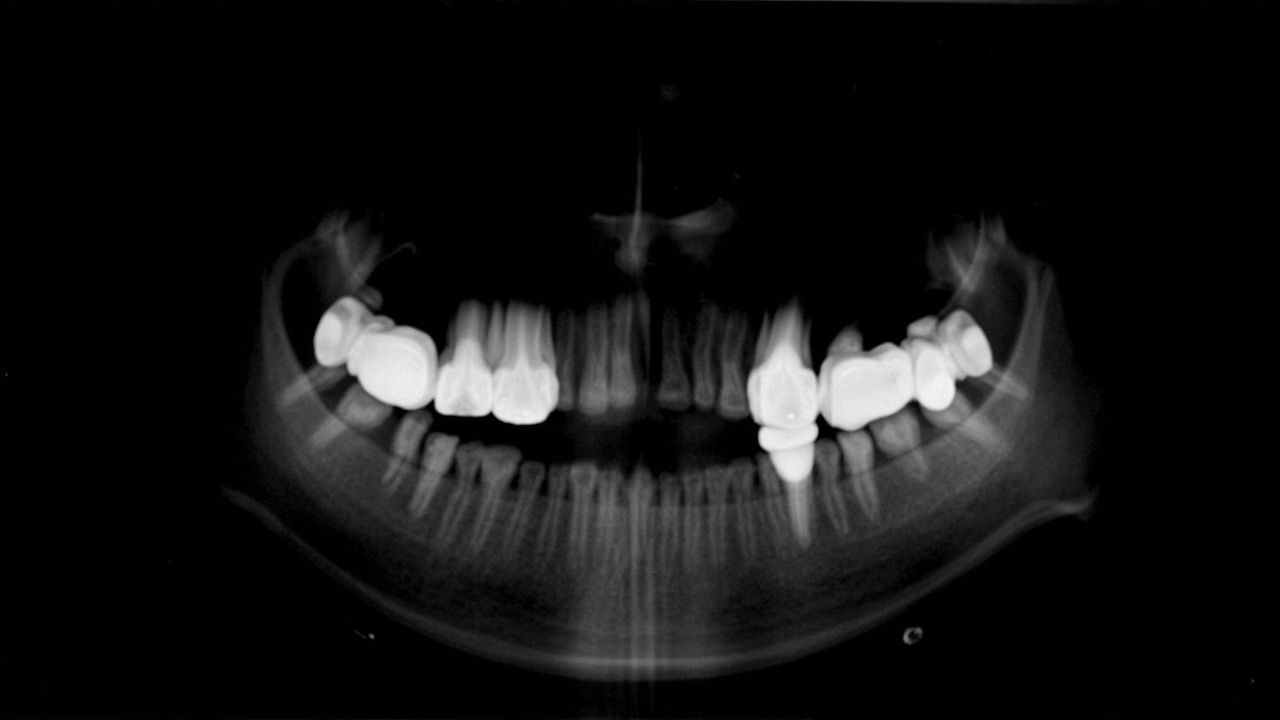
Imaging
Panoramic radiograph (OPG): This single wide X-ray captures all teeth, including the wisdom teeth, and both TMJ structures. It is the first-line imaging for evaluating wisdom tooth position, impaction, and root development. It also shows the overall jaw joint anatomy.
Cone Beam CT (CBCT): If more detail is needed — particularly for evaluating complex wisdom tooth impaction near the inferior alveolar nerve, or for assessing TMJ bony architecture — a CBCT scan provides 3D images at significantly lower radiation than medical CT.
MRI: MRI is the gold standard for evaluating the TMJ disc position and the surrounding soft tissues. It is typically ordered when internal derangement is suspected and conservative management has not resolved symptoms.
Common Co-Occurrence: Wisdom Teeth and TMJ Together
It is entirely possible — and more common than you might expect — to have both a wisdom tooth problem and a TMJ disorder at the same time. This is not coincidence; the two conditions can actually contribute to one another.
How Wisdom Teeth Can Aggravate TMJ
When a lower wisdom tooth is impacted or partially erupted, the inflammation in the surrounding gum tissue triggers a protective muscle response called guarding. The brain tells the jaw muscles to avoid using the affected side, which often means shifting the jaw to one side during chewing. This asymmetrical loading of the TMJ — using one joint more than the other — can strain the joint over time and potentially accelerate disc wear.
Additionally, pericoronitis pain can cause people to clench their jaw unconsciously as a protective response, increasing pressure on the TMJ and potentially triggering or worsening a TMJ disorder.
How TMJ Can Contribute to Wisdom Tooth Symptoms
When TMJ pain causes a person to alter their chewing patterns — favoring one side of the mouth — the increased pressure on the opposite side's molars can trigger symptoms in a wisdom tooth that would otherwise be quiet. TMJ-related tooth grinding (bruxism) also increases pressure on all teeth, including the hard-to-clean wisdom teeth, potentially accelerating decay.
The Clinical Implication
This is why a comprehensive jaw pain evaluation must consider both structures. Removing a problematic wisdom tooth will not automatically resolve TMJ pain if an underlying TMJ disorder is present. Similarly, treating TMJ with a night guard will not resolve pain caused by pericoronitis. Both conditions need to be identified and addressed in their own right.
Treatment Approaches for Each Condition
Treatment for Wisdom Tooth Pain
Pericoronitis (mild to moderate):
- Saltwater rinses (warm salt water, 2–3 times per day)
- Irrigation under the gum flap by a dentist
- Antibiotics if bacterial infection is present
- Pain management with NSAIDs (ibuprofen or naproxen)
- Soft food diet until symptoms resolve
Pericoronitis (recurrent or severe) or impacted wisdom tooth:
- Wisdom tooth extraction (surgical removal) is the definitive treatment
- Extraction is typically performed by an oral surgeon under local anesthesia, sedation, or general anesthesia
- Recovery: 3–7 days of swelling and discomfort; full healing of the socket takes 2–3 weeks
Tooth decay in wisdom tooth:
- Filling if the decay is accessible and the tooth is functional
- Extraction if the decay is extensive or the tooth is inaccessible
Treatment for TMJ Pain
First-line (conservative) treatments — appropriate for most TMD cases:
-
Custom night guard or occlusal splint: A dentist-made acrylic guard worn at night reduces clenching force and protects the joint surfaces. Unlike over-the-counter boil-and-bite guards, custom guards are precisely calibrated to your bite. (Learn more about choosing a night guard for jaw clenching)
-
Physical therapy for the jaw: A physical therapist trained in orofacial rehabilitation can provide targeted jaw exercises, manual therapy to release tight muscles, and posture correction. Research in the Journal of Oral Rehabilitation consistently shows physical therapy as one of the most effective treatments for TMJ myofascial pain. (Browse our guide to the best jaw massagers for at-home TMJ relief)
-
Stress management: Mindfulness-based stress reduction, cognitive behavioral therapy, and relaxation techniques reduce the unconscious clenching that drives most TMJ disorders.
-
Medications: Short-term NSAID use, muscle relaxants, or low-dose tricyclic antidepressants (for chronic TMJ pain) may be prescribed by your dentist or physician.
-
Diet modification: Eating soft foods, avoiding chewing gum, and cutting food into small pieces reduces joint load during the healing phase.
Second-line treatments (if conservative care fails after 6–12 months):
- Arthrocentesis (joint irrigation with sterile fluid to reduce inflammation)
- Arthroscopic surgery (minimally invasive joint surgery)
- Open joint surgery (for severe structural damage)
- Total joint replacement (extremely rare, reserved for end-stage joint destruction)
When to Seek Emergency Care
Some jaw pain symptoms require prompt evaluation. Seek emergency dental or medical care if you experience:
- Severe jaw swelling that spreads to the neck or floor of the mouth — this can indicate a spreading dental infection (odontogenic cellulitis) that can compromise the airway
- Difficulty swallowing or breathing alongside jaw swelling — this is a medical emergency
- Fever combined with jaw pain and gum swelling — suggests active infection
- Jaw locked open or locked shut — cannot be reduced without professional intervention
- Sudden, severe jaw pain after an injury or dental procedure — possible fracture or dry socket
- Numbness of the lip, chin, or tongue — possible nerve injury or involvement requiring urgent evaluation
Frequently Asked Questions
How can I tell if my jaw pain is from wisdom teeth or TMJ?
The key difference is location and behavior. Wisdom tooth pain typically radiates from the back of the mouth — the upper or lower third molar area — and is often accompanied by swollen gums, visible eruption through the gum line, or pain that worsens when eating hard or chewy foods near the back teeth. TMJ pain originates at the jaw joint itself (in front of the ear) and is more likely to be associated with jaw clicking or popping, difficulty opening the mouth fully, and pain that spreads to the temple, ear, or neck. X-rays and a clinical examination by a dentist are the only definitive way to differentiate them.
Can wisdom teeth cause TMJ pain?
Yes, impacted or partially erupted wisdom teeth can contribute to TMJ pain. When a wisdom tooth fails to emerge properly, it creates localized inflammation in the surrounding gum tissue. This inflammation and the associated muscle guarding (clenching to avoid using the painful area) can strain the TMJ over time. Additionally, a wisdom tooth that erupts at an angle can alter your bite alignment, which may increase pressure on the TMJ disc.
When should I see a dentist for jaw pain?
See a dentist within one to two weeks if jaw pain persists beyond a few days without a clear cause, if you notice swelling in the jaw or face, if you have difficulty opening your mouth wider than two finger-widths, if jaw pain is accompanied by fever or signs of infection, or if you experience jaw locking (inability to open or close fully). If your jaw pain is severe and sudden — particularly after dental work or injury — seek emergency dental care within 24 hours.
Do all wisdom teeth need to be removed?
Not all wisdom teeth require removal. Wisdom teeth that are fully erupted, positioned correctly, able to be cleaned properly, and not causing pain or disease can often be retained. However, impacted wisdom teeth (those that fail to fully emerge due to lack of space) have a high risk of causing problems and are commonly recommended for extraction. Your dentist will assess your specific situation using panoramic X-rays to evaluate the position, angle, and root development of all four wisdom teeth.
What is the TMJ disc and how does it affect jaw pain?
The TMJ disc is a small pad of cartilage that sits between the ball and socket of the jaw joint, acting as a cushion that allows smooth jaw movement. When this disc slips out of its normal position — a condition called disc displacement — it can cause clicking or popping sounds, catching sensations when opening or closing the mouth, and eventually cartilage breakdown that leads to arthritis in the joint. Disc displacement is a hallmark of TMJ disorders and is not related to wisdom teeth.
Can TMJ pain be treated without surgery?
The vast majority of TMJ disorders — estimated at 90 to 95 percent — are successfully managed without surgery using conservative treatments. These include physical therapy exercises, custom night guards to reduce clenching, stress management techniques, anti-inflammatory medications, jaw stretches, and heat or cold therapy. Surgery is reserved for cases where structural damage to the joint (such as bone deterioration or severe disc displacement) has not responded to 6 to 12 months of conservative treatment.
Sources & Methodology
- National Institute of Dental and Craniofacial Research (NIDCR). (2024). Temporomandibular Joint Disorders (TMD). Retrieved from https://www.nidcr.nih.gov
- American Association of Oral and Maxillofacial Surgeons. (2023). Management of Impacted Wisdom Teeth: Clinical Guidelines. Retrieved from https://www.aaoms.org
- Scrivani, S.J., Matthews, D.A. & K. Esposito, K. (2023). Temporomandibular Joint Disorders. New England Journal of Medicine, 388(24), 2277–2288.
- Dolwick, M.F. & K. Dimitroulis, G. (2024). The Role of Arthrocentesis in the Management of TMJ Disc Displacement Without Reduction. International Journal of Oral and Maxillofacial Surgery, 53(2), 112–119.
- American Dental Association. (2024). Evaluation and Management of Third Molar (Wisdom Tooth) Pathology. Retrieved from https://www.ada.org
- University of Edinburgh / NHS Health Scotland. (2024). Pericoronitis: Clinical Features and Management. Oral Health Guidance Series.
About the Author
Dr. Rachel Torres, DDS is a board-certified oral and maxillofacial surgeon with fifteen years of clinical experience in the diagnosis and surgical management of wisdom tooth pathology and temporomandibular joint disorders. She earned her Doctor of Dental Surgery degree from the University of Southern California and completed her oral and maxillofacial surgery residency at the University of Texas Health Science Center at Houston. Dr. Torres has published research on the relationship between third molar impaction and TMJ symptomatology in the Journal of Oral and Maxillofacial Surgery. She practices in Austin, Texas, and serves as a clinical instructor at the Texas A&M College of Dentistry.
Last updated: July 2026 | This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.