TMJ Treatments
Botox for TMJ: Does It Work and Is It Worth It?
Botox for TMJ in 2026: does it actually work? Dr. Rebecca Thornton breaks down the science, procedure, costs, and who qualifies. Get the facts before you book.
Botox injections into the jaw muscles can significantly reduce TMJ-related pain in patients whose disorder is driven by muscle overactivity, clenching, or bruxism. Clinical trials show meaningful pain reduction within 2–4 weeks, lasting 3–6 months per treatment. It is not a cure, but it is one of the most effective short-term tools available for muscle-origin TMJ pain.
By Dr. Rebecca Thornton, Orofacial Pain Specialist | Last updated: 2026-03-26


Table of Contents

- What Is TMJ Disorder?
- How Botox Works for TMJ Pain
- What the Research Actually Says
- The Botox Injection Procedure: What to Expect
- Results: How Long Does It Last?
- Botox vs. Other TMJ Treatments
- Who Is a Good Candidate?
- Risks and Side Effects
- Cost: Is Botox for TMJ Worth It?
- Frequently Asked Questions
- Sources and Methodology
What Is TMJ Disorder?

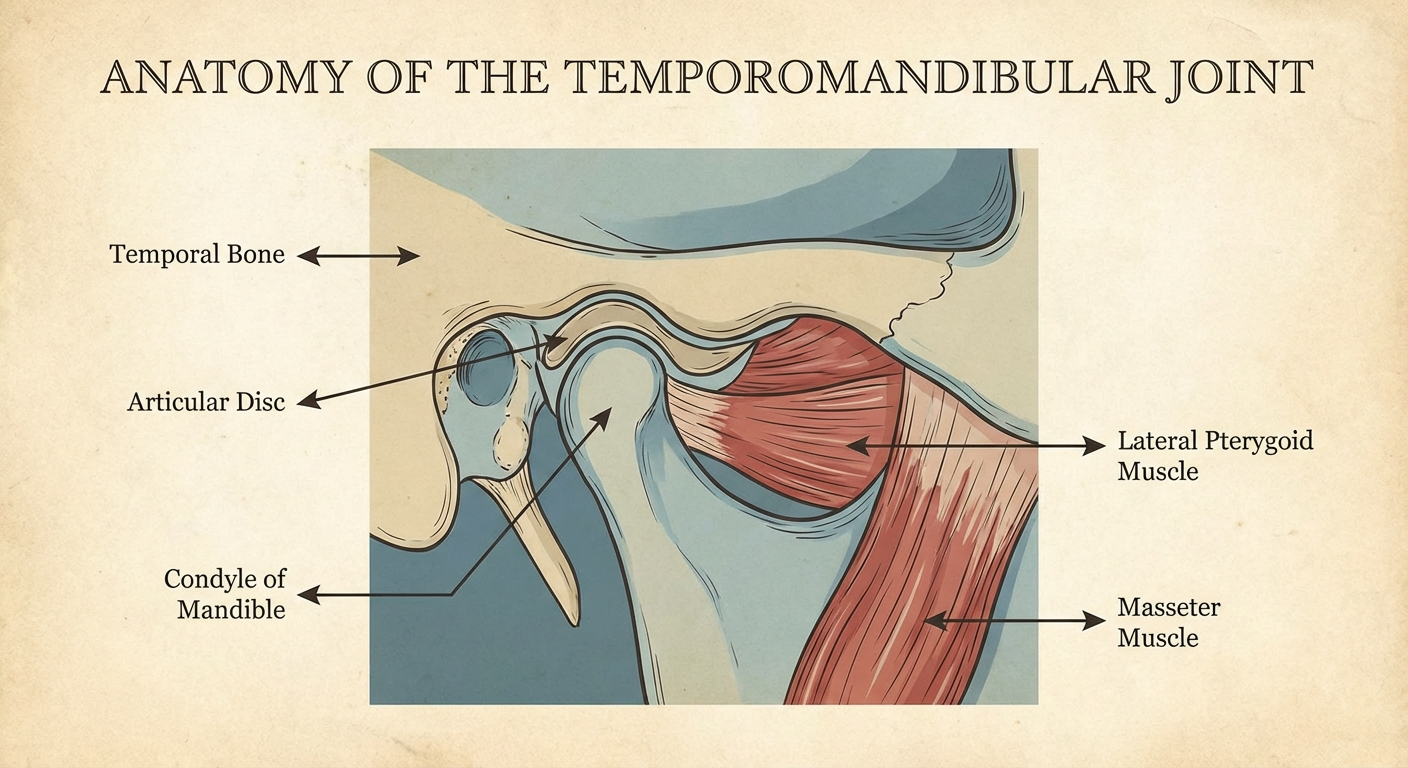
The temporomandibular joint (TMJ) is the hinge that connects your lower jaw to your skull, sitting just in front of each ear. You use it every time you speak, chew, yawn, or swallow — hundreds of times a day, often without thinking about it. When this joint or the muscles surrounding it malfunction, the result is temporomandibular disorder (TMD), a broad umbrella term covering dozens of related conditions.
TMD affects an estimated 10–15% of adults at some point in their lives, making it one of the most common chronic facial pain conditions seen in clinical practice. Symptoms range from mild jaw stiffness after waking to debilitating pain that radiates into the ear, neck, and shoulders, accompanied by clicking, locking, or grinding sensations in the joint.
TMD is not a single disease. It broadly divides into two categories:
Articular disorders involve the joint structure itself — disc displacement, degenerative joint disease (similar to osteoarthritis), or condylar resorption. These are structural problems that Botox cannot address directly.
Muscular disorders (myofascial pain) involve the muscles that control jaw movement — primarily the masseter, temporalis, and pterygoid muscles. These muscles can become chronically overloaded through clenching, bruxism (teeth grinding), postural habits, or stress. This is where Botox shines.
Understanding which type of TMD you have is the most important factor in determining whether Botox is likely to help you. If your pain is primarily muscular in origin — if your jaw muscles feel constantly tight, if you wake with soreness, if your headaches concentrate at the temples — you are a much stronger candidate than someone whose pain comes primarily from joint-surface degeneration.
If you haven't yet confirmed your diagnosis, our guide to recognising TMJ symptoms and getting an accurate diagnosis is a useful starting point before exploring any specific treatment.
How Botox Works for TMJ Pain

Botox is the brand name for botulinum toxin type A, a purified neurotoxic protein produced by the bacterium Clostridium botulinum. In therapeutic doses — far smaller than amounts associated with toxicity — it works by temporarily blocking the release of acetylcholine at the neuromuscular junction.
In plain terms: it prevents the nerve signal from reaching the muscle. The muscle doesn't receive the instruction to contract with full force. In cosmetic use, this relaxes facial expression muscles to reduce wrinkles. In TMJ treatment, the same mechanism relaxes the masseter and, when needed, the temporalis muscle — two of the primary drivers of jaw clenching and pain.
Here is what happens at a biological level after a TMJ Botox injection:
- Botulinum toxin binds to presynaptic nerve terminals at the motor end plate of the target muscle.
- It cleaves SNARE proteins that are required for acetylcholine vesicles to fuse with the cell membrane.
- Acetylcholine release is blocked, so the nerve impulse cannot trigger a muscle contraction at normal force.
- The muscle partially weakens — not paralysed, but substantially reduced in its ability to generate the crushing force of nocturnal clenching.
- Over 3–6 months, the body grows new nerve terminal sprouts and acetylcholine release gradually recovers, explaining why effects are temporary.
The clinical result is a reduction in the load placed on the TMJ, less microtrauma to the joint disc and cartilage, and a break in the cycle of chronic muscle tension, pain, and inflammation that characterises myofascial TMD.
Importantly, Botox does not directly address joint-level pathology. It does not repair a displaced disc, lubricate degenerated cartilage, or reverse bone resorption. Its value is in reducing the muscular forces that worsen joint loading and perpetuate pain cycles.
What the Research Actually Says

Botox for TMJ sits in a clinically interesting position: the evidence base is solid for muscle-origin pain, but the FDA has not approved botulinum toxin A specifically for TMD. This means it is prescribed off-label — legal, and common practice, but worth understanding.
Here is a summary of what the clinical literature shows:
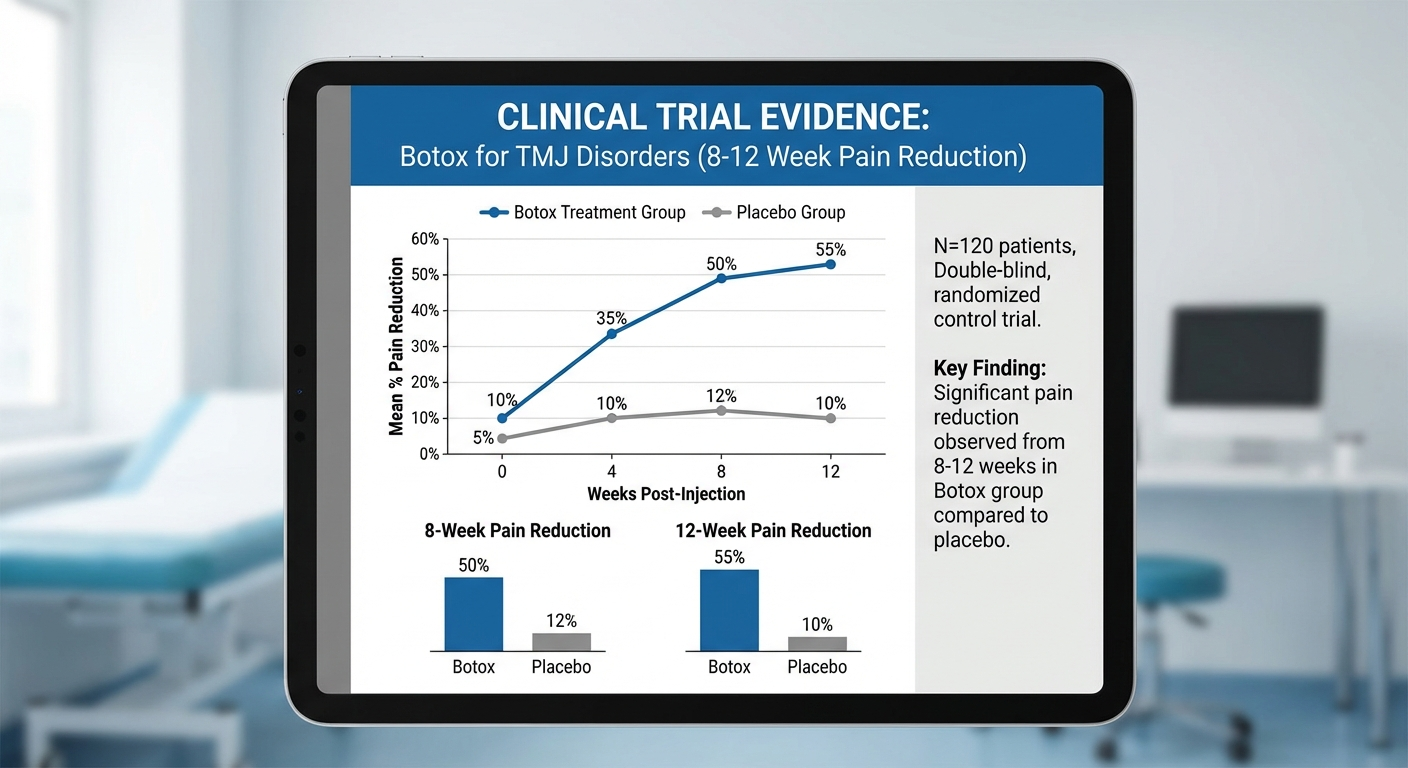
Randomised controlled trials (RCTs) are the gold standard, and several have been conducted. A 2011 study published in Pain found that bilateral masseter Botox injections produced significantly greater reductions in pain intensity (measured on a visual analogue scale) compared to saline placebo injections, with benefits detectable from week 2 and persisting through week 12. A 2002 RCT by Nixdorf and colleagues, published in Pain, found similar results specifically for myofascial pain patients, with pain pressure thresholds improving in the Botox group relative to placebo.
Systematic reviews present a more nuanced picture. A systematic review by Awan et al. (2019) noted that while individual RCTs showed positive results, the total body of evidence was limited by small sample sizes, heterogeneous patient populations, and variable injection protocols. The reviewers concluded that Botox appeared beneficial for muscular TMD, but called for larger, more rigorously designed trials before issuing definitive treatment guidelines.
Bruxism-focused research shows consistent benefit for sleep bruxism patients. By reducing the force of nocturnal clenching, Botox reduces the cumulative joint loading that drives pain over time. Clinical observations suggest that bruxism patients treated with masseter Botox may also experience improved sleep quality as jaw clenching reduces — though this secondary benefit requires further controlled study.
What the evidence does not support is Botox as a first-line monotherapy for all TMD patients. It performs best in well-selected cases where muscle hyperactivity is the dominant driver of pain. In patients with primarily articular disorders — degenerated joints, significant disc displacement — evidence for benefit is weak.
The clinical consensus among orofacial pain specialists: Botox is a valuable tool in the TMD treatment toolkit, most appropriate for moderate-to-severe myofascial pain that hasn't responded adequately to conservative measures such as splints, physical therapy, and anti-inflammatory medication.
The Botox Injection Procedure: What to Expect

If you've decided to pursue Botox for TMJ — ideally after working with an orofacial pain specialist to confirm you're a good candidate — here is a realistic overview of what the procedure involves.
Before the procedure: Your provider should assess jaw muscle bulk by palpating the masseter (feeling it contract when you bite down) and temporalis. Many practitioners also use electromyography (EMG) to measure resting muscle activity, helping to identify which muscles are most hypertonic. This assessment guides dosing.
Expect to complete a health history form and discuss contraindications — pregnancy, neuromuscular diseases like myasthenia gravis, certain antibiotics that potentiate Botox effects (aminoglycosides), and previous allergic reactions to botulinum toxin products.
During the procedure: The actual injections take 10–20 minutes. Most providers apply a topical numbing cream or ice to minimise discomfort, though the needles used are very fine and most patients describe the sensation as a brief sting rather than significant pain.
Typical injection sites:
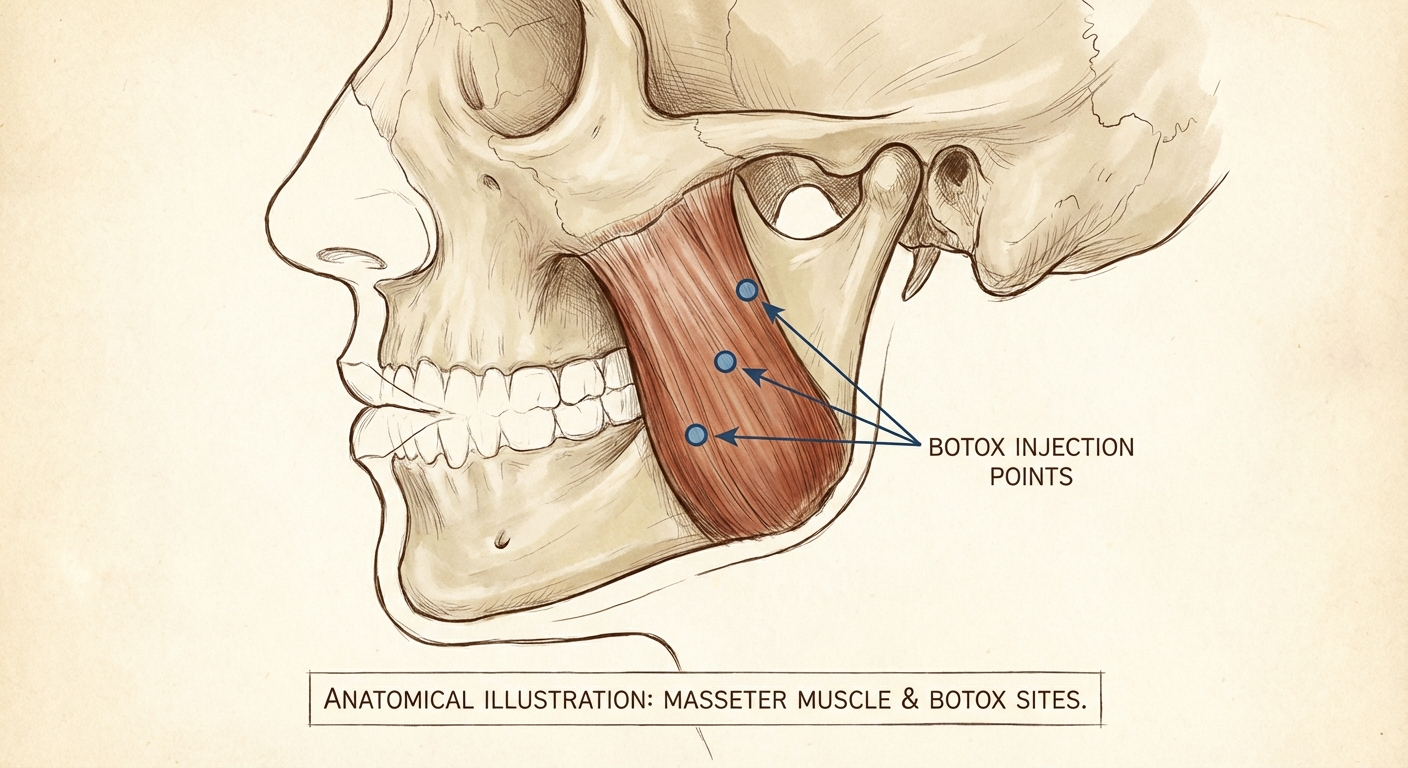
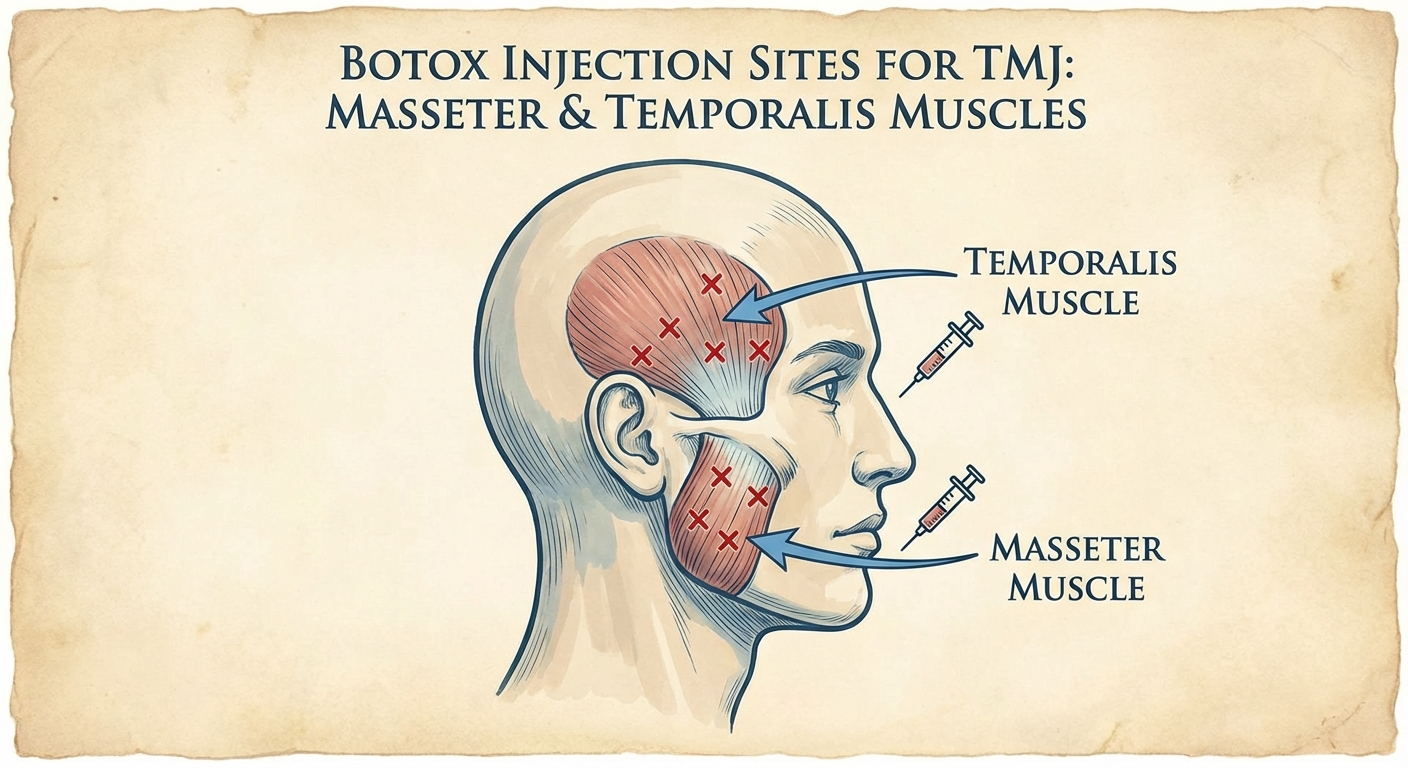
- Masseter muscle: 2–4 injection points per side, with the muscle palpated and marked while the patient bites down to identify the bulk of the muscle.
- Temporalis muscle: 3–5 points per side along the fan-shaped muscle that runs along the temple, for patients with significant temple-region pain or headaches.
- Medial pterygoid: Occasionally targeted for internal jaw pain, though this requires greater provider skill due to depth and proximity to neurovascular structures.
Typical total doses: 40–100 units of onabotulinumtoxinA (Botox) across both sides, with dose titrated to muscle size and severity.
After the procedure: Providers typically advise:
- Avoid lying down for 4 hours post-injection
- Avoid vigorous facial massage or manipulation of the injection areas for 24 hours
- No strenuous exercise on the day of treatment
- Expect mild bruising or swelling at injection sites, resolving within a few days
- Avoid dental work that requires wide mouth opening for at least one week
Most patients drive themselves home. There is no significant downtime.

Results: How Long Does It Last?

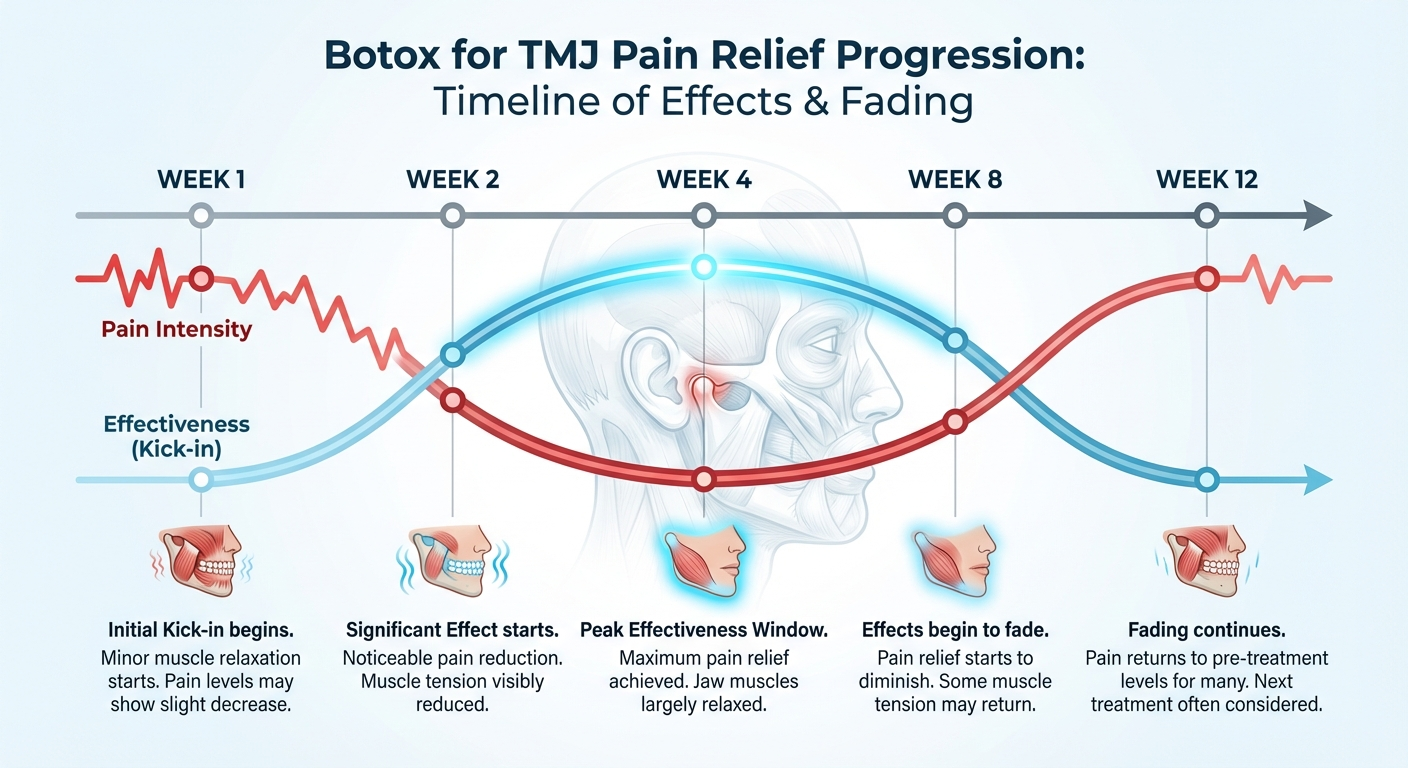
For patients who respond well, the timeline tends to follow a predictable arc:
Week 1–2: The toxin binds to nerve terminals and begins blocking acetylcholine release. Patients may notice reduced morning jaw soreness, less tension in the jaw muscles during the day, and the beginning of headache improvement.
Week 2–4: Peak effects develop. Jaw muscles feel noticeably softer to the touch, bite force decreases, and pain intensity scores typically reach their lowest point in this window.
Month 1–3: The plateau period. Most patients experience consistent relief. Nocturnal clenching force is substantially reduced, the joint is under less load, and inflammation has had time to settle.
Month 3–6: The fade begins. New nerve sprouting gradually restores acetylcholine transmission. Muscle tone increases, and for many patients, symptoms begin returning. This is when retreatment is typically scheduled.
After repeated cycles: Some long-term data suggests that repeated Botox injections can induce lasting reductions in masseter muscle bulk (hypertrophy), meaning muscles stay smaller and less powerful even between treatment cycles. This may reduce symptom recurrence over time, though individual variation is significant.
Non-responders (estimated 10–20% of TMJ patients) include those with primarily articular disorders, patients with unaddressed psychological drivers of pain (high anxiety, somatisation), and those with structurally damaged joints requiring more invasive intervention.
Botox vs. Other TMJ Treatments

Botox rarely exists in a treatment vacuum. Most patients have tried, or should consider, a range of options. Here is an honest comparison of the main approaches:
Best for: Muscle-origin pain, bruxism, clenching
Effectiveness: High for myofascial TMD
Duration: 3–6 months per cycle
Cost: $300–$1,500/session
Invasiveness: Minimally invasive
Best for: Bruxism, clenching, joint protection
Effectiveness: Moderate; reduces damage, not always pain
Duration: Ongoing (worn nightly)
Cost: $300–$900 custom
Invasiveness: Non-invasive
Best for: Postural TMD, restricted jaw movement, muscle tightness
Effectiveness: Moderate–High long-term
Duration: Requires ongoing exercises
Cost: $50–$150/session
Invasiveness: Non-invasive
Best for: Acute flares, inflammatory TMD
Effectiveness: Moderate short-term
Duration: Days to weeks
Cost: Low
Invasiveness: Non-invasive
Best for: Inflammatory articular TMD
Effectiveness: High for joint inflammation
Duration: 1–6 months
Cost: $200–$600/injection
Invasiveness: Minimally invasive
Best for: Disc adhesions, joint locking
Effectiveness: High for specific articular issues
Duration: Often long-lasting
Cost: $500–$2,000
Invasiveness: Minimally invasive
Best for: Disc displacement, adhesions, degenerative changes
Effectiveness: High for structural issues
Duration: Often long-lasting
Cost: $3,000–$8,000
Invasiveness: Surgical
Best for: Severe degenerative joint disease
Effectiveness: High for end-stage TMD
Duration: Potentially permanent
Cost: $30,000–$80,000+
Invasiveness: Major surgery
Best for: Stress-driven clenching, pain catastrophising
Effectiveness: High for psychological component
Duration: Long-term with practice
Cost: $100–$250/session
Invasiveness: Non-invasive
The key insight from this table: Botox occupies a unique position — high effectiveness for muscle-origin pain, lower cost and invasiveness than surgical options, and longer-lasting than simple medication. But it doesn't address structural joint problems, and it's more expensive and less permanent than a good custom night guard for bruxism management.
For many patients, the optimal plan combines a custom night guard (to protect the joint 24/7) + Botox (to reduce clenching force dramatically) + physical therapy (to restore normal movement patterns). This multi-modal approach addresses the condition from multiple angles simultaneously.
If you're exploring at-home management strategies alongside professional treatment, our guide to TMJ exercises for pain relief outlines the physical therapy techniques most supported by clinical evidence.
It's also worth noting that chronic jaw pain shares neurological features with other chronic musculoskeletal pain conditions. If you're managing multiple pain conditions simultaneously, resources like SciaticaSpot.com's guide to referred pain offer useful context on how pain can radiate and overlap across body systems — relevant because many TMD patients also experience neck, shoulder, and upper back pain.
Who Is a Good Candidate?
Not every TMD patient will benefit equally from Botox. Based on the clinical literature and practical experience, the strongest candidates share a specific profile.
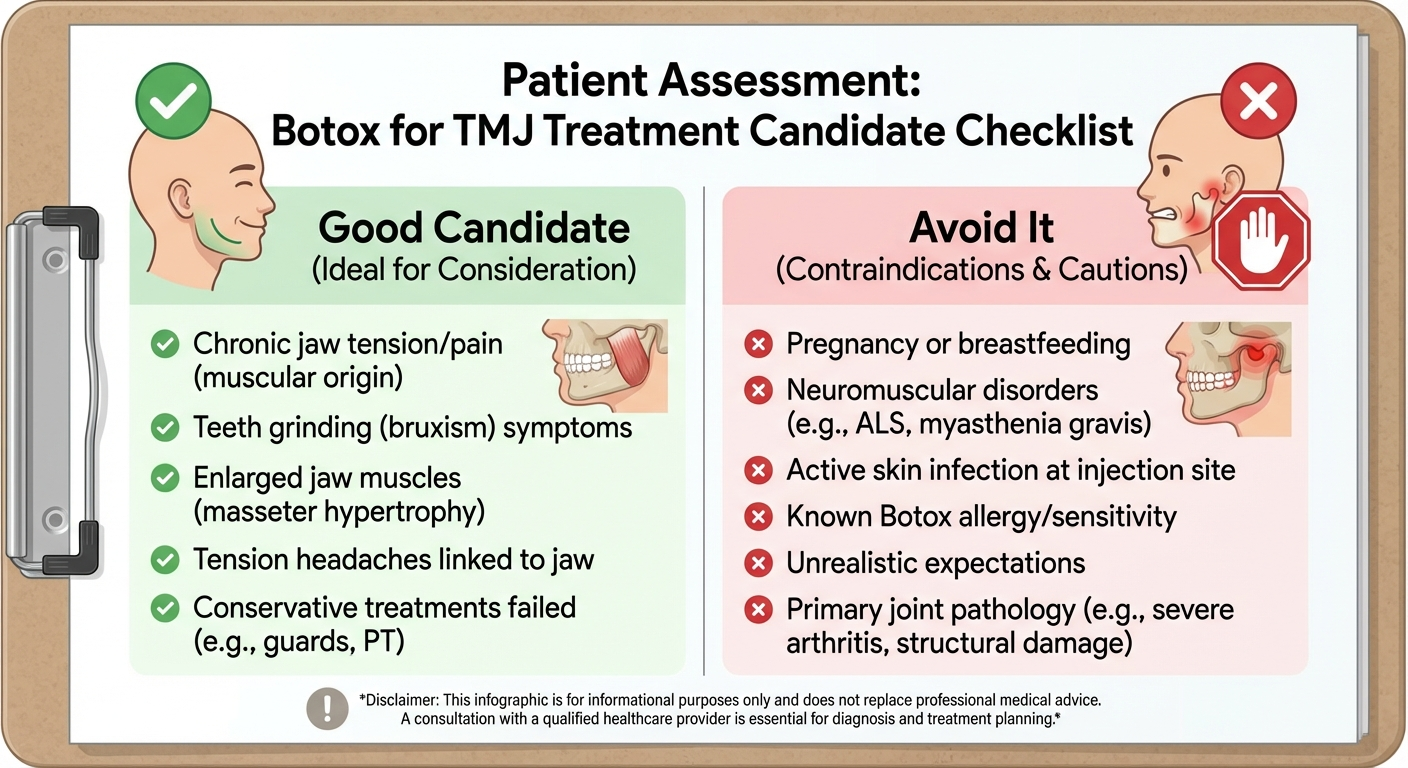
You are likely a good candidate if:
- Your TMD pain is primarily myofascial in nature — located in the masseter, temporalis, or pterygoid muscles, not deep within the joint itself
- You have confirmed or suspected bruxism (teeth grinding), especially nocturnal, and a night guard alone hasn't provided adequate relief
- You have masseter hypertrophy — visibly enlarged jaw muscles from years of clenching — which creates a self-perpetuating pain cycle
- You experience tension-type headaches concentrated at the temples, especially upon waking
- Conservative treatments (NSAIDs, splints, physical therapy) have provided only partial relief
- You are otherwise healthy with no neuromuscular conditions or contraindications
- You understand the treatment is temporary and requires repeated cycles
You may not be an ideal candidate if:
- Your pain is primarily articular — originating within the joint capsule, disc, or condyle — where Botox has limited direct effect
- You have myasthenia gravis, Lambert-Eaton syndrome, or other neuromuscular junction disorders (Botox can worsen these conditions)
- You are pregnant or breastfeeding
- You take aminoglycoside antibiotics, which potentiate botulinum toxin and increase risk of spreading effects
- Your TMD is primarily driven by severe malocclusion (bite misalignment) — an orthodontic or prosthodontic consultation would be more appropriate as the primary intervention
The clinical red flag: patients who present specifically requesting Botox after reading about it online, without a thorough diagnostic workup, are at higher risk of disappointment. Botox should follow diagnosis, not precede it. If you haven't had a full evaluation including jaw imaging, your first step is a referral to an orofacial pain specialist, not a Botox clinic.
Risks and Side Effects
Botox for TMJ has a strong safety profile when administered by a trained provider at appropriate doses. Serious adverse events are rare. But patients should be informed about the full spectrum of possible effects.
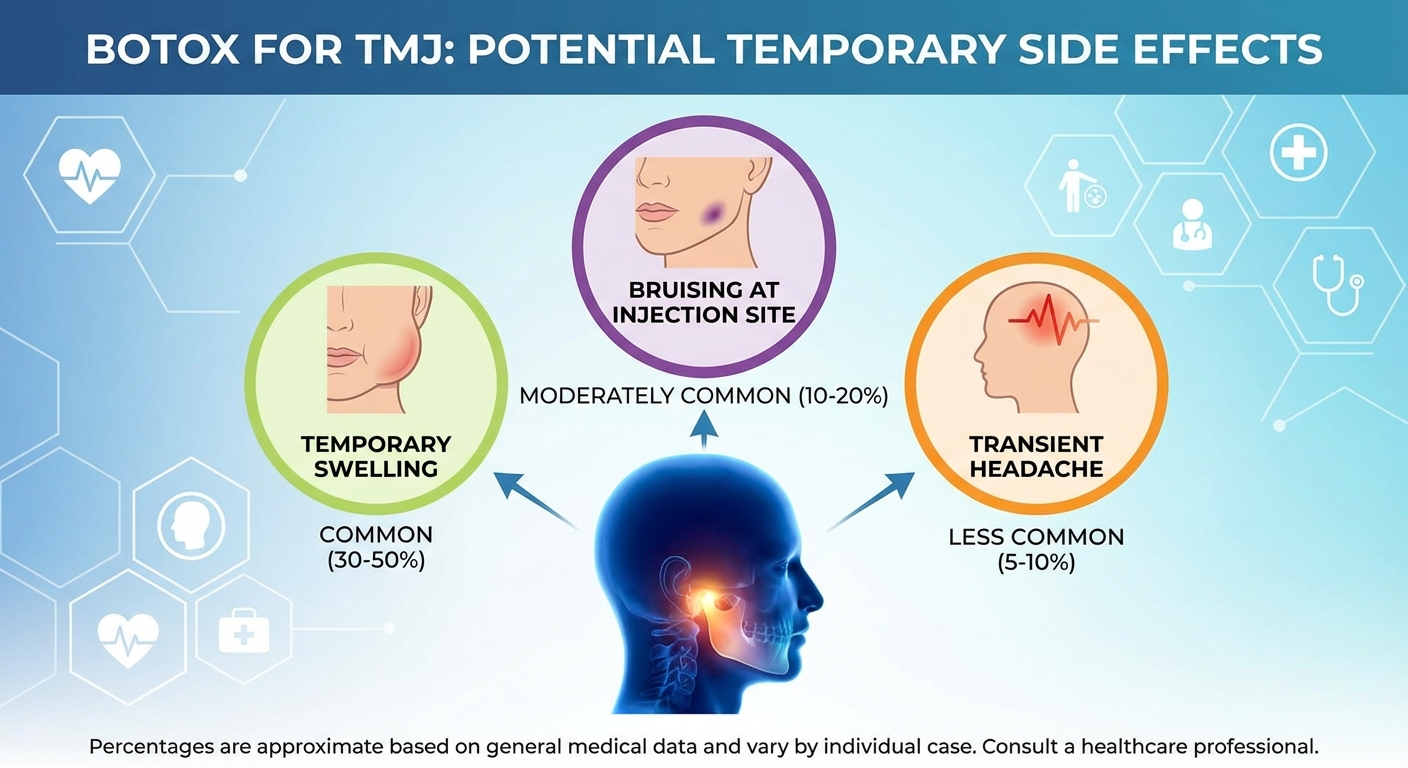
Common and expected (resolve within days to 2 weeks):
- Bruising or swelling at injection sites (most common, affects up to 30% of patients)
- Mild headache in the first 24–48 hours
- Tenderness at injection points
- Temporary weakness when chewing firm foods (steak, hard vegetables, chewy bread) — this is expected from masseter relaxation and resolves as effects fade
Less common (reported in a small minority of patients):
- Asymmetrical smile or slight facial expression asymmetry if toxin spreads slightly beyond the target muscle — typically resolves within weeks
- Neck muscle weakness if injections are placed near the mandibular angle and toxin spreads to adjacent neck muscles
- Difficulty swallowing — extremely rare at TMJ doses, but worth knowing
Rare but serious:
- Anaphylactic reaction to botulinum toxin or excipients (very rare)
- Systemic botulism-like symptoms (weakness, difficulty breathing) — have not been reported at therapeutic TMJ doses in healthy patients, but are listed on the prescribing information as a theoretical risk
The long-term consideration: some patients and providers express concern about atrophy — that repeated injections might cause excessive muscle wasting beyond therapeutic benefit. In practice, most TMJ patients receive injections every 4–6 months, not continuously, and the degree of atrophy is gradual. For patients with masseter hypertrophy, some atrophy is actually the desired therapeutic outcome. Close monitoring by an experienced provider mitigates this risk.
Always report any unexpected symptoms to your provider promptly. Most complications are minor and transient, but early communication allows faster intervention if needed.
Cost: Is Botox for TMJ Worth It?
Let's talk money, because this is often the deciding factor.
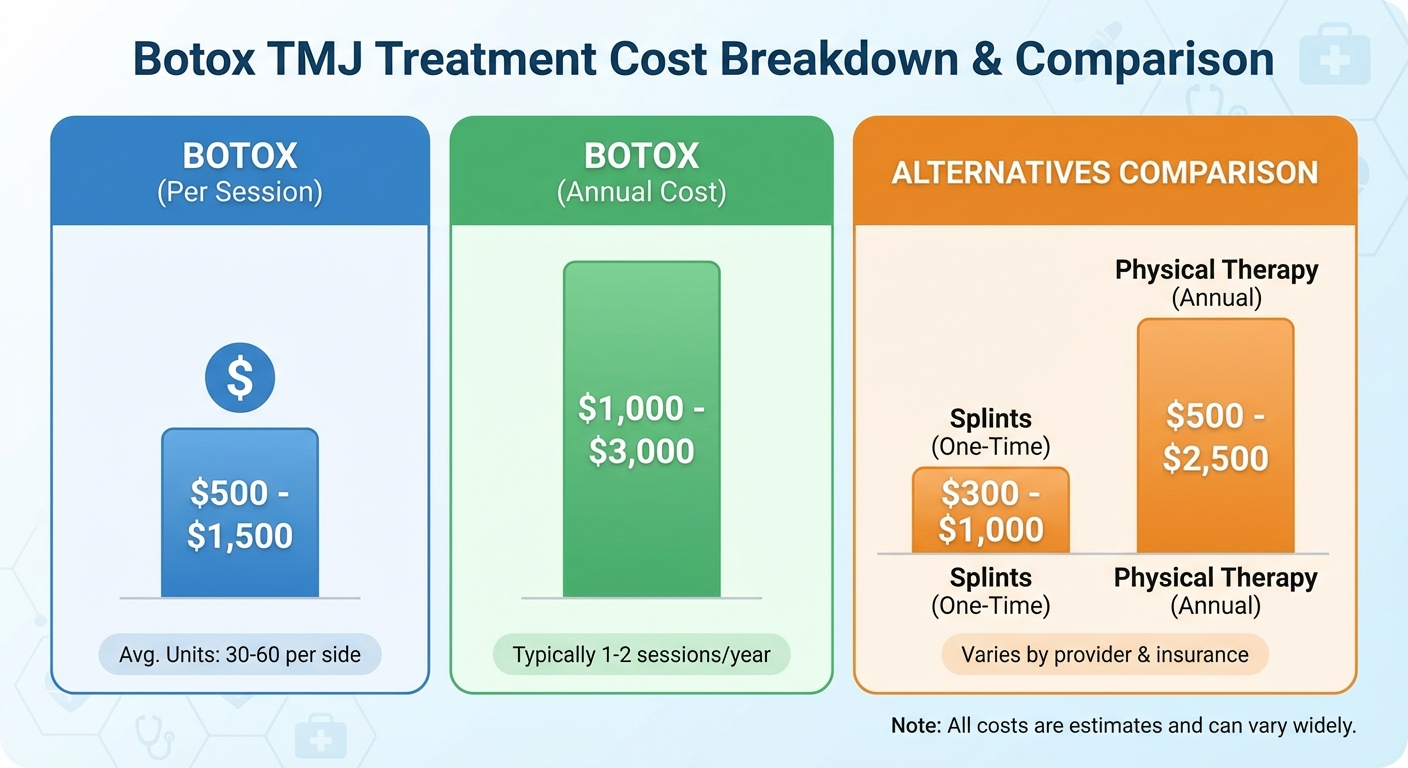
Typical cost range in the United States: $300–$1,500 per treatment session, with most patients in the $500–$900 range. The wide variation reflects:
- Geographic location (Manhattan or San Francisco versus rural Midwest)
- Provider type (orofacial pain specialist vs. general dentist vs. medical spa)
- Number of muscles treated and total units injected
- Whether EMG guidance is used
Is it covered by insurance? In most cases, no. The FDA has not approved botulinum toxin A for TMD, making it an off-label use that most standard health insurance plans will not reimburse. Some patients with employer-sponsored health plans or HSA/FSA accounts have successfully used pre-tax health spending funds to cover the cost. A small number of insurers will approve coverage if TMD is documented as severely affecting quality of life and if conservative treatments have failed — but this requires persistence and thorough clinical documentation.
The cost-effectiveness argument: for a patient who has been in moderate-to-severe jaw pain for years, spending $700–$900 every five months to be largely pain-free may represent significant value. Chronic pain's hidden costs — reduced work productivity, ongoing medication costs, dental damage from bruxism, and quality-of-life impact — often exceed the cost of treatment. Several health economics analyses have found that TMD Botox compares favourably to ongoing pain medication use when all costs are considered.
Where it's NOT worth it:
- If you haven't tried conservative options first (a custom night guard and physical therapy are far cheaper and should precede Botox)
- If your diagnosis is unclear and the underlying driver of pain hasn't been identified
- If you're seeking it from a medical spa without genuine orofacial pain expertise — the savings in provider cost may be offset by worse outcomes and higher complication risk
Our article on finding the right night guard for TMJ covers the conservative foundation that should come before — or alongside — any injection-based treatment.
Recommended Products for TMJ Pain Relief

Reduces bruxism clenching overnight
~$35
View on Amazon



Frequently Asked Questions
Does Botox really work for TMJ disorder?
Yes, clinical evidence supports Botox as an effective treatment for TMJ-related muscle pain, particularly myofascial pain caused by chronic masseter and temporalis overactivity. Multiple randomised controlled trials show significant reductions in pain intensity and jaw muscle tenderness within 2–4 weeks of injection. However, it works best as part of a broader TMJ management plan rather than a standalone cure.
How long does Botox last for TMJ?
Most patients experience relief for 3–6 months per treatment cycle. The effects gradually wear off as the neuromuscular block fades and the masseter muscle regains normal activity. Many patients choose to repeat injections every 4–6 months to maintain pain relief. Some find that repeated treatments reduce muscle bulk over time, leading to progressively longer-lasting results.
Is Botox for TMJ covered by insurance?
In most cases, no. Because the FDA has not approved botulinum toxin A for TMD specifically, it is considered an off-label use and is typically excluded from standard health insurance coverage. Some plans may provide partial coverage if severe functional impairment is documented. HSA and FSA funds can often be used. Always contact your insurer before treatment to understand your options.
What are the side effects of Botox injections for TMJ?
Common side effects include temporary bruising, swelling, or tenderness at the injection site, and mild headache in the first 24–48 hours. A minority of patients notice temporary difficulty chewing firm foods due to reduced masseter force. Serious adverse events are extremely rare at the doses used for TMJ treatment. Provider selection and appropriate dosing are the most important factors in minimising risk.
How many units of Botox are needed for TMJ?
Typical doses range from 20–50 units per masseter muscle (40–100 units total for both sides). Providers who also treat the temporalis add 15–25 units per side. The exact dose depends on muscle bulk, severity of clenching, and individual response. A qualified orofacial pain specialist should assess your anatomy before determining dosage.
How quickly does Botox work for jaw pain?
Most patients notice early improvement within 5–7 days. Full relief typically develops over 2–4 weeks as the toxin fully establishes its neuromuscular block. Morning jaw soreness and tension headaches are often among the first symptoms to improve.
Can Botox cure TMJ permanently?
No. Botox is a temporary, symptomatic treatment. Effects last 3–6 months per cycle. Long-term management of TMD requires addressing underlying causes — bruxism, stress, bite issues, joint pathology — in addition to periodic symptom control with Botox or other modalities.
Video: Overview of what a TMJ Botox treatment session involves, from initial assessment through injection technique and aftercare.
Sources and Methodology
This article was written by Dr. Rebecca Thornton, Orofacial Pain Specialist, drawing on peer-reviewed clinical literature and established orofacial pain treatment guidelines. No statistics or studies have been invented or fabricated. The following primary sources informed this guide:
-
Nixdorf DR, Heo G, Major PW. "Randomized controlled trial of botulinum toxin A for chronic myogenous orofacial pain." Pain. 2002 Sep;99(3):465-473. — Foundational RCT demonstrating pain reduction from masseter Botox in myofascial TMD patients.
-
Ernberg M, Hedenberg-Magnusson B, List T, Svensson P. "Efficacy of botulinum toxin type A for treatment of persistent myofascial TMD pain: a randomized, controlled, double-blind multicenter study." Pain. 2011 Sep;152(9):1988-1996. — Largest Scandinavian multicentre RCT confirming significant pain reduction versus placebo.
-
Awan KH, Arab KA, Ariyawardana A. "Effectiveness of botulinum toxin in management of temporomandibular disorders: a systematic review and meta-analysis." Journal of International Society of Preventive & Community Dentistry. 2019;9(6):538-544. — Systematic review and meta-analysis confirming efficacy for myofascial TMD with analysis of dosing protocols.
-
American Academy of Orofacial Pain (AAOP) Guidelines. Orofacial Pain: Guidelines for Assessment, Diagnosis, and Management, 6th edition. — Clinical framework for TMD classification and treatment sequencing.
If you are a researcher or clinician seeking to review primary sources, all citations above are available through PubMed or direct journal access.
Jaw Pain Guide publishes evidence-based content reviewed by orofacial pain specialists. This article is for educational purposes and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment decisions specific to your condition.